Knee surgery
There are many types of surgery that can be performed on the knee. Some of the more common operations are detailed here.
Knee revision
The mechanisms of failure of knee are fairly similar although obviously not identical to that of the hip. These include infection, deep infection, loosening, wear, peri-prosthetic fracture and rarer causes of failure include dislocation.
Deep infection
The principles of dealing with deep infection of the knee are very like that of the hip joint although in this country the concept of revising the knee in one operation is slightly less common but gaining popularity.
The principles are to open the knee, remove all infected material and implants, to thoroughly wash the knee out and to insert a temporary spacer which can be made from a mould in the form of cement which will release antibiotics, quite commonly Vancomycin, into the tissues to give very high tissue concentrations.
The knee is stitched up and the patient is allowed to mobilise with this articulating spacer. It does not allow anything like normal movement but it does allow the soft tissue envelope to keep open and the muscles active. At a later date when the parameters of infection, normally the blood tests measuring the ESR and C-reactive Protein, come down to normal and the clinical status allows a second operation, the second stage is carried out. This involves opening the knee, removing the articular spacer and then re-inserting a new knee prosthesis. On these occasions, it may be necessary to use a more constrained or linked knee and have more extended fixation to cope with the bone loss that may ensue.
X-ray showing a knee with an articulating cement spacer (AP view).

X-ray showing a knee with an articulating cement spacer (lateral view).

X-ray showing the same patient after revision surgery using a rotating hinge knee replacement and bone grating to the tibia contained with metal mesh (AP view).

X-ray showing the same patient after revision surgery using a rotating hinge knee replacement and bone grating to the tibia contained with metal mesh (lateral view).

Knee Wear
Wear is a function of loss of the polyethylene on the tibial side and in the same way as the hip this polyethylene debris then causes a cellular reaction of the macrophages and the macrophages release cytokines or small chemicals which further cause bone resorption in effect melts the bone away from the cement of the prosthesis causing a secondary loosening process. It is dealt with in a similar manner to loosening.
Loosening
Loosening can occur because of the wear process of polyethylene or just the mechanical repetitive loads on the interface.
This can cause fairly substantial bone loss around the lower part of the femur and upper part of the tibia and because of this it is no longer possible in many occasions to allow simple condylar or surface fixation and therefore it is necessary to use larger stems to go down the upper femur and down the tibia which are usually cemented in place although some cementless fixation is possible.
Bone loss can be addressed by using bone graft, particularly on the tibial side as it can on the hip.
Peri-prosthetic fractures
Peri-prosthetic fractures can occur around the knee just as they can around the hip.
Again, if the knee replacement is loose it is necessary to treat the fracture and revise the knee at the same sitting.
If the fracture is above the fixation bed one can just treat the fracture.
Total Knee Replacement (TKR)
In many regards the operation of total knee replacement has lagged behind that of total hip replacement by a period of about ten years and therefore as total hip replacement surgery took off in the early 1960s and early 1970s, successful knee replacement was delayed some ten years or so.
Initially, the attempts to replace the knee were fairly conservative using surface replacements as Charnley did in the hip but these implants lost the fixation in many cases and therefore the concept of replacing the whole articular surface as Charnley did in the hip was accepted.
Early pioneers included Michael Freeman from the London Hospital and John Insall, also an Englishman who went to work at the Hospital for Special Surgery in New York.
The results of the early total knee replacements of condylar fixation, condylar design and fixed with cement have been very good and success rates in the region of 95 per cent at ten years have been achieved. The knee is exposed; the joint surfaces are trimmed back using special jigs to allow the surgeon to accurately realign the knee. More recently computer techniques have been used to assist the surgeon.
Image showing a condylar design of total knee replacement with the three components, the highly polished metal femoral component, the metal tibial component and the polyethylene tibial tray.

Unicompartmental or Partial Knee Replacement
Quite often (about 20 per cent of cases) the arthritis predominantly affects just the inside of the knee, so-called medial compartment of the knee - the inner side.
As a result, the outer or lateral side of the knee and the articulation between the back of the kneecap and the femur, the patella femoral joint is reasonably well preserved. It therefore seems logical just to resurface the damaged portion of the knee.
The early failures of the localised surface replacement were probably a product of poor design and relatively poor fixation. Although some surgeons continued with medial or unicondylar replacement they were in the minority.
Over the last ten years this procedure has increased in popularity. This has mainly been because of published outcomes which are reasonable (although inferior to total knee in terms of lasting ten years). The realisation that patients often have better knee function with a unicompartmental knee has contributed to the growing popularity of this procedure.
There are two main design types, the so-called “mobile bearing” implant where the polyethylene is allowed to move and slide on top of the metal tibial tray and the “fixed” design in which the polyethylene tibial tray is fixed onto the metal tibial tray. The advantage of mobile bearing type is to reduce stresses on the implant due to the congruent articulation, therefore reducing wear of the polyethylene.
The principles of surgery are similar to total knee arthroplasty although it is possible to use a much smaller incision to insert the implants using jigs by removing just the articular surfaces of the femur and tibia. The functional outcomes are almost certainly better in patients having localised replacements. The longer-term outcomes defined as how long they last in large Registry series such as the Swedish Arthroplasty Register would indicate that the failure rate due to loosening is about double that of total knee replacements and benchmark figures for 10-year survivorship of total knees are in the region of 95 per cent. Therefore, although the functional results are better they are slightly less robust. These issues need to be discussed with the patient and this potential trade off discussed in terms of implant selection.
The concept of replacing just the medial side of the knee has extended to replacing the outer side of the knee if there is a deformity on the outer side of the knee and also between the kneecap and the patella if the joint is localised, patello-femoral replacement.
Implants & bearings
Since the initial success of Sir John Charnley in developing hip replacement at Wrightington Hospital there has been a huge amount of research and development in joint replacement technology. There is now an enormous variety of hip and knee replacement designs available utilizing different fixation methods, materials and bearings. In the following pages, some of the more important aspects of prosthetic design are discussed.
Design
The Charnley hip or low frictional torque arthroplasty - LFA - has quite specific design features.
Charnley relied on the femoral stem to get good fixation to the bone using acrylic bone cement and also used a high-density polyethylene socket which was also cemented into the acetabulum.
The unique features of this design is the small head compared to the normal femoral head. The diameter of femoral head is quite commonly 50 to 54mm however Charnley used a diameter of 7/8inch or 22.225mm.
The reasons for this are mainly due to wear, friction and lubrication. The articulation is mainly dry and is not reliant on joint fluid and a bearing which is small has a low or short sliding distance, i.e. the amount of plastic the femoral head runs over as the hip moves backwards and forwards from side to side and it is this low sliding distance which causes relatively low wear of the hip.
The second reason for using a small femoral head was that this imparts a relatively low torque on the interface between the socket and the bone due to the relatively low ratio of the head diameter to the external diameter of the socket. It was for these reasons that Charnley used a small femoral head. Subsequently some surgeons were concerned about the dislocation potential of this design and therefore subsequent attempts have been made to increase the diameter of the femoral head.
Other types of design principles relate to the geometry of the stem whether it be a flat stem, a tapered stem, a textured stem. The stem is to be fixed to the bone either with bone cement or with cementless fixation. It is now generally accepted for cementless stems that of a tapered polished design produces reliable long term results.
This was mainly the philosophy of the Exeter group of surgeons and is the design of the Exeter stem from Robin Ling and Clive Lee. However, other cemented designs have quite a rough surface. They have a different design principle in that the stems are essentially held up and fixed rigidly whereas the tapered designs do allow some movement or engagement of the femoral stem and load the cement under compression. There are therefore two quite different but both acceptable design principles of design and fixation of the stem to the bone.
In terms of the acetabular component, high density polyethylene is still used although there are newer generations of the polyethylene to make it more wear resistant and this can be achieved by cross linking the polyethylene by using radiation during the manufacturing process.
The newer cross linked polyethylenes show very low wear properties, maybe an 80 per cent reduction in wear although there is slight concern regarding a reduced mechanical strength of the material although these risks are probably very low indeed. Certainly, in the United States there is an increase usage of these cross link polyethylenes.
By increasing the wear resistance of the polyethylene, it is therefore possible to increase the diameter of the femoral head without introducing grossly adverse wear environments and this has led to a reintroduction of larger femoral head designs.
If the femoral head is larger, the potential advantages are greater stability of the joint, potentially a greater functional range of movement before the hip impinges on the acetabular bone and therefore potentially better function. There is some evidence that the larger femoral head has a lower dislocation potential.
Fixation
Robust fixation of implants is very important as in younger patients these joints are required to last 20 to 30 years or even more.
Charnley used a material called acrylic bone cement to fix the implants to the bone which had previously been used by dental surgeons and this material can still be very effective. The bone cement is made by mixing a fluid component with a powder component and the liquid becomes doughy within a few minutes, becomes like putty within about four of five minutes and most cements set around the ten-minute mark.
The exact setting characteristics of the cement do differ somewhat depending on the different types of materials used in the bone cement. So, some bone cements can set quite quickly in five minutes and others can set over a longer period over 15 minutes. Once set the cement is very strong under compression and forms a very good bond between the prosthesis whether it be the femoral component or acetabular component or indeed the femoral component of a knee replacement or tibial component of a knee replacement. Various histological studies and long term follow ups show that this bone cement can maintain excellent fixation over many years.
X-ray showing a cemented Charnley total hip replacement which has been functioning well for 28 years and still shows no signs of wear or loosening.

However, other innovators have used uncemented fixation, that is a fixation not reliant on bone cement and in uncemented fixation the surgeon creates an accurate shape within the bone to accept the component which is press-fit. Bone grows into the surface of the component over a period of normally 12 weeks or so.
The surface of the components is often textured or microstructured or porous to allow bone to grow into the surface of the implant (although this is not always the case) and some designers advocate a surface coating, normally hydroxyapatite which is bone inductive, in other words encourages the bone to grow onto or into the implant.
There has been a general trend over the last five to ten years to use more uncemented devices and this is probably reflective in improved designs and to some extent better surfaces and perhaps in relation to hydroxyapatite.
Particularly with the hip, some surgeons advocate using a cemented stem and uncemented acetabulum - this is termed hybrid fixation.
Ceramic
Ceramics are crystalline structures either based on Alumina and sometimes Zirconia and sometimes composite materials. They are extremely hard and wear resistant. They are also quite critical in terms of manufacturing and the potential downside of ceramic is that they are quite sensitive to crack propagation and very rarely fracture. However, having said that the risks of fracture in most well designed ceramic bearings are very low but there have been occasions where fractures have occurred.
Ceramic can be used against a high-density polyethylene or cross link polyethylene or it can be used articulating on a ceramic counterpart on the acetabulum. More recently the combination of ceramic articulating with a metal acetabular component has been looked at in the hip.
Theoretically, experimentally and clinically the ceramic on ceramic bearing probably produces the least wear of any articulation and the ceramic debris is very inert in the body and therefore has been used more recently and more frequently, particularly in the UK. The slight downside to ceramic is a very low fracture risk in the region of 1 in 10,000 or so and a small incidence of squeaking that can occur with a ceramic on ceramic articulation.
Ceramics articulating on ceramic have been used for many years on the continent and very good results have been obtained at 10, 15 years. Newer types of ceramics such as Delta ceramic have yet to be fully assessed but theoretically may be better materials.
Metal-on-metal
The metal-on-metal coupling produces significantly less wear than a metal on polyethylene coupling. Typical average volumetric wear from a standard metal femoral head of 28mm diameter articulating with a plastic socket is in the region of 80 cubic millimetres per year and in comparison, the wear from a metal on metal joint is in the region of 1 cubic millimetre per year. Ceramic wear is about 10-fold less.
Although the volumetric wear is considerably less the particles are quite small, in the region of a nanometre compared to microns from the polyethylene.
A local tissue reaction from these metal particles is generally much less than the polyethylene although as the particles are smaller they can travel to distant parts of the body. This may be good or it may be bad. It may be good because as the particles are transported away from the articular surface and from the joint they may cause less damage to the fixation of the implant and therefore causing a dilution of the effects. However, the long-term accumulation of this metal is unknown. However, about 80 per cent of the metal plus is excreted in the kidneys.
Lubrication regimes of a metal on metal implant are very different from the metal on plastic implants. The large surface areas and very small clearances, that is the gap or different radius or diameter of the femoral component to the acetabular component can allow fluid entrapment and therefore achieving a different lubrication regime - hydrodynamic lubrication versus the boundary lubrication of a dry joint.
If fluid is allowed to ingress and is maintained, then theoretically the metal surfaces are separated and therefore wear becomes minimal. It is more likely that part hydrodynamic and part boundary lubrications exist in these metal metal joints.
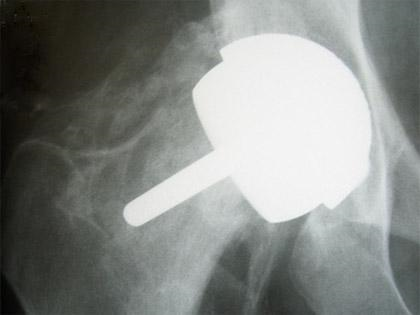
The metal-on-metal combination can be used as a resurfacing or in combination with a standard femoral stem with a large femoral metal head articulating with a metal socket.
X-ray showing Birmingham hip resurfacing.

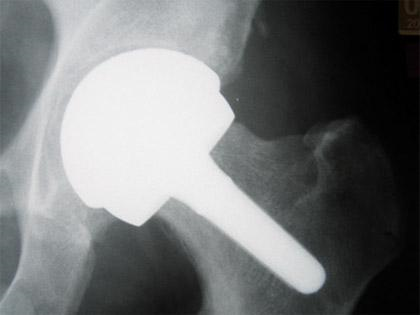
X-ray showing standard femoral stem with large metal head articulating with metal socket.

X-ray showing a Birmingham Mid Head Resection. The larger stem on the femoral component can be seen in comparison to the standard resurfacing.
X-ray showing fracture of the femoral neck in a patient with a hip resurfacing. Heterotopic ossification (new bone formation) has also occurred around the hip.